Catholic Candle note: Catholic Candle usually focuses directly on Faith and morals. However, sometimes issues in society have a severe indirect impact on Faith and morals and should be addressed. Below, we examine one of those issues which has a severe indirect impact on Faith and morals, viz., the overblown corona-scare. We put COVID-19 in perspective, to help readers face this challenge in which Providence placed us, for the glory of God and for our good.
In our current corona-crazy world, people are acting strangely because they are frightened by (supposed) imminent death from COVID-19, or they are intimidated by abusive governmental lockdown orders.
People have been coerced into failing to gather to sanctify the Sunday together (which is important, even in the present Great Apostasy, when we have no Masses and no uncompromising priests, at least in most places in the world). People have been bludgeoned into letting go of their humanity and are fearfully acting as if their fellow man was a threatening virus-culture rather than a fellow child of God and fellow soldier in the Church Militant.
Lastly, another reason to examine the exaggerated corona death toll is because it is a prominent example showing (for anyone who needs further proof) that the mainstream media is unreliable as a source of the truth concerning what is going on in the world. It is Catholic Candle’s hope that this present article is a helpful reminder to our readers that they should distrust the mainstream media because it lies and “spins” the truth.
This article uses the statistics which were current when the article was written in August and September, 2020. The article mostly uses data from the U.S. because there is so much of this data available. For the most part, we do not include the data from the rest of the world because that information is less available to us and also in order to avoid this article becoming too cumbersome.
However, the data we have from other countries supports the theses of this article. That support makes sense because human nature is the same in all countries, COVID-19 is (apparently) the same everywhere, and the lockdowns are broadly similar, although more severe and abusive in some places than in others.
There are three aspects to the COVID-19 (so-called) “pandemic”, which help us to put the “COVID-19 death” totals in perspective:
1. COVID-19 is in the same “ballpark” with (and has the same fatality profile) as the annual flu;
2. The collateral deaths caused by the government lockdowns likely greatly exceed the deaths caused by COVID-19, even if the inflated COVID-19 death tolls were the true ones; and
3. The COVID-19 death numbers are unreliable and inflated.
Below, we examine each of these points.
1. COVID-19 is in the same “ballpark” with (and has the same fatality profile) as the annual flu
There are almost no deaths of younger and healthier people. For example, the latest CDC numbers (from August 15, 2020) show 309 deaths of persons 24 years of age and younger.[1] More than 90% of COVID cases are asymptomatic and people usually don’t know they ever had the virus.[2]
Almost all persons who were listed as “COVID-19 deaths” were retirement age (65 or older), especially over 85 years old.[3] Almost all of them (94%) had co-morbidities, meaning they were being treated for something else which was a known lethal condition.[4]
In fact, the persons who were counted as “COVID deaths” had an average of 2.6 co-morbidities – meaning that more than half of them had three co-morbidities (compared to the number who had 2 co-morbidities).[5]
A person who receives only the slanted,
deceptive news of the mainstream media would not be aware of the truth
concerning the relative lack of danger for most people. Instead, people are given
the impression that everyone is in great danger of dying at any time from
COVID-19. A recent Gallup poll reveals how ignorant and scared the American
people are (because of the mainstream media’s and Democrats’ fear-mongering).
Look at these two graphs of Gallup Poll results, comparing reality and
misperception:

This graph is found here: https://www.franklintempleton.com/investor/article?contentPath=html%2Fftthinks%2Fen-us-retail%2Fcio-views%2Fon-my-mind-they-blinded-us-from-science.html

This graph is found here: https://www.franklintempleton.com/investor/article?contentPath=html%2Fftthinks%2Fen-us-retail%2Fcio-views%2Fon-my-mind-they-blinded-us-from-science.html
Despite the false perception promoted by the mainstream media and the Democrats, the reality is that COVID-19 is in the same “ballpark” with, and has the same fatality profile as the annual flu, viz., it is usually something that does not affect most people and, if it does affect us, it is usually a little “blip” in our month. (See, the two graphs above.) However, older people in poor health have to take extra precautions for COVID-19, just like they should regarding the annual flu.
To put this in perspective, there were 80,000 U.S. fatalities in the 2017-2018 annual flu season, and this number was so unremarkable that this death toll passed virtually unnoticed at the time.[6]
No one was locked down in 2017-2018 because of 80,000 flu deaths. The economy was not destroyed because of that annual flu. There were no masking orders, no churches closed, and no other oppressive government orders. In a country the size of the U.S., with over 330 million people, a lot of people die every day and every year.
Not only is the current COVID-19 scare overblown, but even now, some years of the annual flu, e.g., 1968, have killed more people per capita than COVID-19. https://www.thelancet.com/journals/lancet/article/PIIS0140-6736(20)31201-0/fulltext (We do not even mention the far-worse 1918 flu season.)
It goes without saying that in none of those years – which were worse than the current year – was there a lockdown or other over-reaction, such as we see in the current year.
2. The collateral deaths caused by the government lockdowns likely greatly exceed the deaths caused by COVID-19, even if the inflated COVID-19 death toll were the true one
In the section above, we saw that COVID-19 is in the same “ballpark” with (and has the same fatality profile as) the annual flu, viz., it is usually something that does not affect us and if it does affect us, it is usually a little “blip” in our month. However, older people in poor health (especially with multiple co-morbidities) have to take extra precautions for COVID-19, just like they should regarding the annual flu.
That older, sicker persons are in a different situation than the general population, is underscored by the fact that 42% of all U.S. “COVID-19 deaths” occur in nursing homes, although those facilities contain only 0.62% of the U.S. population.[7]
In the U.S., the states controlled by the (more liberal) Democratic party locked down more severely their general populations of younger and healthier people (compared to Republican states). However, the Democratic governors of four of these states killed thousands of their most vulnerable people (who were in nursing homes) by forcing those nursing homes to receive other persons who tested positive for COVID-19.[8]
This is exactly the opposite of what should have happened! Younger, healthier people should have been allowed to go on with their lives, while the government should have allowed nursing homes to protect the most vulnerable people, like those nursing homes protect their residents every year from the annual flu.
Self-inflicted harm and the deaths from delayed medical care, during the corona-isolation
Among the many severe tolls taken by the corona-scare is the increases of suicides, drug overdoses, and deaths from delayed care for other serious illness because of the draconian corona-lockdowns.
It is obvious to any person of common sense that the severe lockdowns would cause great collateral harm. Here are how more than 500 doctors described this harm in their public letter to President Trump:
It is impossible to overstate the short, medium, and long-term harm to people’s health with a continued shutdown. … Losing a job is one of life’s most stressful events, and the effect on a person’s health is not lessened because it also has happened to 30 million other people. Keeping schools and universities closed is incalculably detrimental for children, teenagers, and young adults for decades to come.
The millions of casualties of a continued shutdown will be hiding in plain sight, but they will be called alcoholism, homelessness, suicide, heart attack, stroke, or kidney failure. … In youths it will be called financial instability, unemployment, despair, drug addiction, unplanned pregnancies, poverty, and abuse.[9]
Johns Hopkins Center for Health Security examined the idea of “Large-Scale Quarantine Measures” in its November 4, 2006 study entitled: Disease Mitigation Measures in the Control of Pandemic Influenza. Here is what that university study concluded:
The negative consequences of large-scale quarantine are so extreme (forced confinement of sick people with the well; complete restriction of movement of large populations; difficulty in getting critical supplies, medicines, and food to people inside the quarantine zone) that this mitigation measure should be eliminated from serious consideration.[10]
Although many people gullibly accept the false narratives of the mainstream
media, we see now – by looking at the results of the lockdowns around us – why
rational studies and doctors (like those quoted above) have rejected/opposed
such lockdowns.
Before discussing the dramatic increase in suicides during the corona-scare, we note that this suicide increase was paralleled by a dramatic increase in help calls to suicide hotlines. Here are some examples of different suicide hotlines with different increases:
➢ Two national hotlines had increases of 47% and 300% respectively.[11]
➢ Another national suicide hotline had a 40% increase.[12]
➢ Another national suicide hotline had an increase of 891% in March 2020, compared to March 2019.[13]
➢ Two other suicide hotlines had an 800% increase in call volume.[14]
These increased suicide “help” calls are attributed by those hotline organizations to “social distancing” and “social isolation” suffered because of the lockdowns.[15]
Indeed, common sense makes predictable the severely negative effects of the lockdowns, because we are human. These lockdowns are inhuman and have never been tried before in the history of mankind: viz., isolate everyone in a nation from all his friends and fellow humans – and isolate each nation throughout almost the entire world. This is rash and foolish in the extreme!
It is no wonder that one of the epidemiologists who advises the British government called the lockdowns a panic response. Here are his words:
Lockdown was a panic measure and I believe history will say trying to control Covid-19 through lockdown was a monumental mistake on a global scale, the cure was worse than the disease. … It was always a temporary measure that simply delayed the stage of the epidemic we see now. It was never going to change anything fundamentally; however low we drove down the number of cases ….
We absolutely should never return to a position where children cannot play or go to school. … I suspect right now more people are being harmed by the collateral effects of lockdown than by Covid-19. …
Any restrictions imposed should be considered measures and should protect those who needed it while letting everyone live more freely. … Instead of concentrating on schools, we should have been concentrating on care homes. We were not really thinking about where the risk lies, just on suppressing the virus.[16]
Regarding the suicide death toll, obviously, the 2020 suicide death toll will not be certain until after the end of 2020. However, the current projection for suicide/drug overdoses deaths is about 150,000 in the U.S.[17] To estimate how many of these deaths are due to the extreme corona-isolation, we subtract the total for the latest year for which there is data: 2018. In 2018, there were 48,344 self-inflicted deaths (suicides and drug overdoses) in the U.S.[18]
Let’s round that 2018 number up to 50,000 deaths. Thus, according to the best projections we have, suicides and drug overdoses in our times of extreme corona-isolation are estimated to be about 100,000 greater this year than before this corona-scare. In other words, self-inflicted deaths are 300% of the 2018 number!
The death toll from COVID-19 is extremely inflated, as we see in section three of this article. However, this death toll is supposedly estimated to be about 183,000. One way to put this supposed death toll in perspective, is that if we take this number and subtract the increase in self-inflicted deaths because of the corona-isolation, we get 83,000 (i.e., 183,000 – 100,000 = 83,000). This is approximately the fatality total from the 2017-2018 annual flu which was so unremarkable that this flu death toll went almost unreported then. Yet, politicians over-react in 2020 and ruin the country’s life.
But there is more: What is not evident in the above comparison of the numbers (viz., “COVID deaths” vs. collateral deaths), is that the deaths blamed on COVID-19 are almost entirely of older, retired people with multiple co-morbidities, most of whom are given only a relatively short time to live even without COVID-19. By contrast, the suicide and drug overdose deaths occur in the younger and otherwise healthier people who have a far longer life expectancy. In other words, each “COVID death” represents a far smaller number of years of life lost compared to the suicide/drug overdose deaths.
Of course, we don’t want anyone to die, but we recognize that a sick, older person losing the last year of his life – as tragic as that is – is not the same as a high schooler losing that last 60 years of his life.
Below, we quote how the U.S. Center for Disease Control (“CDC”) sounded the alarm about the current suicide/drug overdose rate for high schoolers during our corona-isolation. These COVID-19 lockdown death tolls are far greater than the corresponding “COVID-19 death” toll:
But there has been another cost that we’ve seen, particularly in high schools. We’re seeing, sadly, far greater suicides now than we are deaths from COVID. We’re seeing far greater deaths from drug overdose that are above that we had as background than we are seeing the deaths from COVID.[19]
Similar spikes in suicide are occurring elsewhere in the world, e.g., in Australia.[20]
Another of the many great harms inflicted by the lockdowns (which are especially extreme in Democratic states) is deaths that occurred because of postponing medical treatment for other diseases, due to the COVID-19 lockdowns. Those lockdown deaths – which would not have otherwise occurred – are from a variety of causes, e.g., heart attacks, strokes, and cancer.
We don’t know of a comprehensive estimated total of non-COVID-19 deaths which would have been prevented, in the absence of the corona-scare and lockdowns. However, here are some datapoints:
➢ Looking at only two of the many types of cancer (breast cancer and colorectal cancer) the National Cancer Institute predicts there will be 10,000 excess deaths in the U.S. over the next 10 years because of pandemic-related delays in diagnosing and treating these tumors.[21]
➢ Looking at only the drop in cancer referrals, admissions, and diagnoses, compared to pre-COVID levels, one study (using what it called “conservative assumptions”) estimated that there will be 33,890 additional (i.e., excess) cancer deaths during the next year, in the U.S. because of that delayed treatment.[22]
➢ Although we do not have non-COVID increased-fatality numbers for the entire country for heart attacks, strokes, diabetes, and Alzheimer’s disease, we did find statistics of percentage increases in deaths (of persons who did not have COVID-19) from these four diseases, in five Democratic states (Massachusetts, Michigan, New Jersey, New York, and Pennsylvania). These five states were among the most extremely locked down. In these states, in March and April 2020, compared to January and February 2020, there was a:
· 96% increase in diabetes deaths;
· 89% increase in heart disease deaths;
· 64% increase in Alzheimer’s disease deaths; and
· 35% increase in stroke deaths.[23]
Also, in New York City (which suffered a more severe lockdown than almost anywhere), there was a 398% increase in heart disease deaths and a 356% increase in diabetes deaths.[24]
With this data, let’s do our best to estimate, in a rough way, how many deaths these percentages (of additional deaths) would mean throughout the United States. Let us use the latest national numbers (from 2018) for these four causes of death and let us suppose those percentage increases in deaths from lockdown-delay-in-treatment were the same nationwide. In other words, let’s use the 2018 national total deaths from each of those four causes, multiplied by the percentage increases given above, to calculate the excess lockdown deaths from each of those four causes.
This formula means that the lockdown-delays-in-treatment caused:
❖ 81,548 additional diabetes deaths (84,946 deaths x 96% = 81,948)
❖ 583,289 additional heart disease deaths (655,381 x 89% = 583,289)
❖ 78,092 additional Alzheimer’s disease deaths (122,019 x 64% = 78,092)
❖ 51,734 additional stroke deaths (147,810 x 35% = 51,734)[25]
Thus, we see, as a “ballpark” number, that the total of these lockdown-delay-in-treatment deaths is 794,663 additional deaths in the United States. Let’s be clear about these numbers. They are only rough. On the one hand, they would seem to be overstated because they use the data of five Democratic states, whereas other (Republican) states exercised a much “lighter touch” in their lockdowns. So, we would expect that the percentages (of increased deaths) in these Democratic strongholds would be higher than in other parts of the country. This would mean that the national percentages for these lockdown-delay-in-treatment deaths would be lower than in those five Democratic states.
On the other hand, these numbers undercount the lockdown-delay-in-treatment deaths in another way: viz., those percentages only pertain to the increased death from four causes. Since there are roughly 100,000 self-inflicted deaths, plus cancer lockdown-delay deaths, and delay-deaths from other causes too, all those numbers should be added to the total of the lockdown-delay deaths from these four causes (794,663) to approximate the additional U.S. deaths. We see similar collateral deaths from corona-isolation in other countries too.[26]
For the present purpose, we are not trying to get an exact number of the collateral, lockdown-isolation deaths. Nor are we saying that we know there are 800,000 additional deaths. Rather, we are pointing out that these collateral deaths from the corona-lockdowns provide a valuable context to our assessment of the current corona-scare.
It is easy to see how the collateral deaths caused by the government lockdowns could easily exceed – even very greatly exceed – that inflated 183,000 COVID death number which is claimed. Moreover, when comparing those collateral “lockdown deaths” with supposed “COVID-19 deaths”, the comparison is even more dramatic when we consider the number of years lost by people, compared to the number of lives lost (as shown above).
Perhaps someone might suppose that the “COVID-19 deaths” would be far more numerous if the governments did not order the harsh lockdowns which caused the huge numbers of collateral deaths. That supposition is false, as will be shown in a future Catholic Candle article. In fact, those lockdowns were unnecessary and did not help.
3. The COVID-19 death numbers are unreliable and inflated
Above, we saw that the collateral deaths caused by the government lockdowns could easily exceed – even very greatly exceed – that inflated 183,000 “COVID-19 death” number which is claimed.
Now, we examine that “COVID-19 death” total and see if it is reliable.
The overcount of “COVID-19 deaths”
There is a huge difference between dying with COVID-19 and dying from (i.e., because of) COVID-19. Let’s illustrate the difference: the CDC estimates that adults will come down with 2-3 common colds every year.[27] With colds being so common, it is common to die with a common cold, even though not because of a common cold. If someone died while he had a common cold, we would not say he “died from the common cold”.
Well, “COVID-19 deaths” are counted to
include anyone who dies with COVID-19 even though not because
of (from) COVID-19. This is similar to counting a person as a “common
cold death” if the person died while he had a common cold.
Here is how Dr. Deborah Birx (coordinator of the coronavirus taskforce)
explained this U.S. method of counting COVID-19 deaths:
There are other countries that if you had a preexisting condition and let’s say the virus caused you to go to the ICU and then have a heart or kidney problem some countries are recording [this] as a heart issue or a kidney issue and not a COVID-19 death. … [In the US] if someone dies with COVID-19 we are counting that as a COVID-19 death.[28]
With this foolishly broad overcounting, which no one ever uses for other sicknesses, there is a greatly exaggerated COVID-19 death toll. There is not only the everyday overcount we would expect, of sick, frail, elderly people who have multiple co-morbidities, who die of something else (like a heart attack, a stroke, cancer, etc.) but who are counted as a “COVID-19 death” because they died with COVID-19.
But there are also striking absurdities which are consistent with this official policy of counting every death as a “COVID-19 death” as long as the person had COVID-19 when he died, e.g.,
➢ A person who died in a motorcycle accident was listed as a COVID-19 death.[29]
➢ A person who died of suicide was listed as a COVID-19 death.[30]
But the COVID-19 overcount is even more exaggerated because a person need not even be known to have COVID-19. Rather, current CDC protocols allow a person to be reported as a “COVID-19 death” as long as there is an assumption that COVID-19 somehow contributed to the death. Here is the CDC’s instruction:
COVID-19 should be reported on the death certificate for all decedents where the disease caused or is assumed to have caused or contributed to death.[31]
Thus, when the death certificate lists COVID-19 on it, the CDC and the mainstream media report the person as if COVID-19 caused that person’s death. For example, here is one instance of this type of falsification (this one from National Public Radio):
Today, more than 6 million Americans have been infected with the coronavirus and some 183,000 have died from it ….[32]
Here is another example of this type of falsification (this one from the Washington Post):
At least 191,000 people have died of the coronavirus in the United States
….[33]
The truth is that the COVID-19 death total is really of people who died in some way connected with COVID-19, but not because of COVID-19. These people did not all have pneumonia-type COVID-19 symptoms, nor were they all even known to have ever had COVID-19.
In fact, the “COVID-19 death” toll includes many people based on statistical suppositions. For example, early on, New York adopted the policy of counting as “COVID-19 deaths” the number of people who died in excess of a statistically average year, even though those people never tested positive for COVID-19 or had any symptoms suggesting COVID-19.[34] The unreasonableness and inaccuracy of this policy is obvious, since “half the time” (even without COVID-19) the fatalities will be above average – maybe even far above average – to offset the other “half” of the years when the death toll is below average.
Perverse financial incentives to count persons as “COVID-19 deaths”
We see (above) that the CDC authorizes hospitals to count as “COVID-19 deaths” all people whom they “assume” had COVID-19 which somehow contributed to the deaths. These assumptions are made more common by the perverse financial incentives pressuring cash-strapped hospitals to “assume” that COVID-19 had some role contributing to patients’ deaths. For example, the U.S. government pays hospitals a 20% premium in Medicare payments if the hospital “assumes” that a patient was a “COVID-19 death”.[35]
Any reasonable person would know that under these circumstances, there will be lots of “assuming” that COVID-19 had some connection to the death. In fact, some whistleblower doctors have publicly complained that their hospitals pressure them to add COVID-19 as an assumed “contributing cause” on their patients’ death certificates.[36]
Summary of this section so far, of the reasons “COVID-19 death” numbers are inflated
The “COVID-19 death” totals are inflated because a person can be counted if:
➢ The person had COVID-19 when he died (regardless of what actually caused his death); or
➢ The person was assumed to have had COVID-19 when he died; or
➢ There was a statistical increase in deaths above the expected average, regardless of how the persons died.
Further, we see (above) that there is a large perverse incentive for hospitals to lie and to say that a person was a “COVID-19 death” so the hospital would get more money.
Let’s try to estimate the true number of persons whose deaths were caused by COVID-19
How do we figure out how many so-called “COVID-19 deaths” were really caused by COVID-19? One way to roughly approximate this number is to consider what COVID-19 is and then look at the CDC numbers.
COVID-19 is a respiratory disease caused by the virus named SARS-CoV-2. The “SARS” in “SARS-CoV-2” stands for “severe acute respiratory syndrome” (which is sometimes also referred to as acute respiratory distress syndrome or adult respiratory distress syndrome).[37]
The CDC explains that sometimes COVID-19 is severe enough that it leads to death by progressing to pneumonia and acute respiratory distress syndrome (ARDS).[38]
Here is another way this causation is stated:
The virus that causes COVID-19 is designated severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2). The major morbidity and mortality from COVID-19 is largely due to acute viral pneumonitis that evolves to acute respiratory distress syndrome (ARDS).[39]
This is why, last spring, the CDC directors used a “case definition of COVID-19 requiring a diagnosis of pneumonia” in an article they wrote for the New England Journal of Medicine.[40]
Thus, let’s look at the death toll of persons whose death certificates at least mentioned pneumonia (regardless of what they died of). In the CDC chart below[41], you see that there are 71,700 persons who died between February 1, 2020 and August 31, 2020, who at least had influenza or pneumonia when they died (regardless of the actual cause of their death).
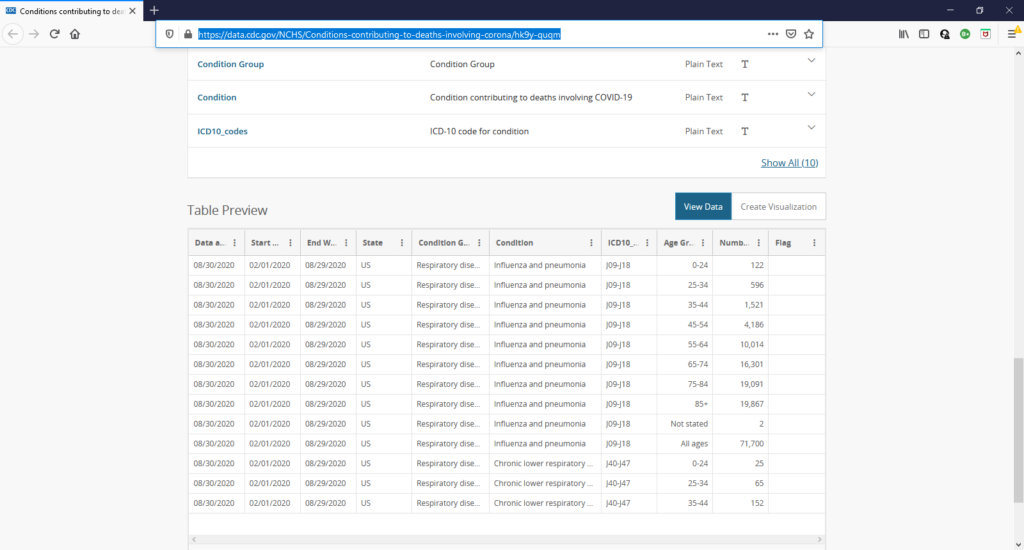
Again, this total is 71,700 deaths. Let’s count that as a rough proxy for how many people with COVID-19 actually died from it, since these people at least had influenza or had the pneumonia which accompanies COVID-19 when people actually die from the disease.
This data is the best we have although, obviously, to the extent that persons had COVID-19 and pneumonia but died of something else, such as a heart attack, these persons would be included in this total and would overcount COVID-19 deaths. Further, to the extent that these persons had influenza and not pneumonia, they also would be an overcount. But let’s “be generous” and count them all, to approximate a real COVID-19 death toll. That number (71,700) is still only 40% of the claimed total of COVID-19 deaths (183,000).
It might seem that 71,700 is a big number. However, the U.S. is a country of 330 million people. In fact, about 2.8 million people die in the U.S. during a typical year.[42]
So, although we don’t want anyone to die, nonetheless pneumonia (and influenza) deaths are currently average for the entire country, not above average. See the current CDC map below.

Map taken from: https://gis.cdc.gov/grasp/fluview/mortality.html
Italy
We could talk about other countries too. However, we will only briefly talk about one other country, Italy, because it has been mentioned so often in the mainstream media’s corona-scare. Italy has the second-oldest population in the world.[43] Just as the annual flu strikes more severely in elderly people with co-morbidities, so does COVID-19 too, as we saw in section one of this article.
However, there is a dishonesty in the reporting of Italy’s COVID-19 fatalities, just as is true in the statistics for the U.S. and other countries. Like for the U.S., the mainstream media attributes to COVID-19 all deaths in which the persons had some connection to the virus. In other words, Italy’s COVID-19 fatality statistics include all the people who died with COVID-19, even when they die of something else and their deaths are not caused by COVID-19.
Here is how this is explained by Prof. Walter Ricciardi, scientific adviser to Italy’s minister of health:
The way in which we code deaths in our country is very generous in the sense that all the people who die in hospitals with the coronavirus are deemed to be dying of the coronavirus. On re-evaluation by the National Institute of Health, only 12 per cent of death certificates have shown a direct causality from coronavirus, while 88 per cent of patients who have died have at least one pre-morbidity – many had two or three ….[44]
Thus, looking at how many people – even among Italy’s more elderly population – have died from COVID-19 as the cause, only 12% of those attributed in Italy as “COVID-19 deaths” showed a “direct causality from coronavirus”. In other words, Italy’s “COVID-19 death” toll is inflated by 800%!
Summary of this article
There are many reasons that it is plain that the corona-scare is overblown. The reality is that:
❖ COVID-19 is in the same “ballpark” with (and has the same fatality profile as) the annual flu;
❖ The collateral deaths caused by the government lockdowns likely greatly exceed the deaths caused by COVID-19, even if the inflated “COVID-19 death” toll were the true one; and
❖ The “COVID-19 death” numbers are unreliable and inflated.
Lastly, beware of the lies and “spin” in the reports of the mainstream media!
[2] See, e.g., https://www.wxyz.com/news/over-90-of-covid-19-cases-in-michigan-treatment-center-are-asymptomatic
[7] https://www.forbes.com/sites/theapothecary/2020/05/26/nursing-homes-assisted-living-facilities-0-6-of-the-u-s-population-43-of-u-s-covid-19-deaths/#2da582ee74cd
[8]
https://www.justice.gov/opa/pr/department-justice-requesting-data-governors-states-issued-covid-19-orders-may-have-resulted
& https://nypost.com/2020/05/16/blame-governors-for-coronavirus-deaths-in-nursing-homes-goodwin/
[9] https://www.scribd.com/document/462339632/ADAD-Letter-Signed#from_embed (emphasis added).
[10] http://www.upmc-biosecurity.org/website/resources/publications/2006/2006-09-15-diseasemitigationcontrolpandemicflu.html (emphasis added).
[12]
https://www.npr.org/sections/health-shots/2020/05/04/847841791/flood-of-calls-and-texts-to-crisis-hotlines-reflects-americans-rising-anxiety
[14] These two hotlines were regional:
➢ In L.A. https://abc7.com/suicide-hotline-calls-coronavirus-covid19-los-angeles/6117099/
➢ In Nashville: https://fox17.com/news/local/feeling-the-pressures-of-the-pandemic-suicide-hotlines-see-800-percent-spike-in-calls
[16] Assessment by Professor Mark Woolhouse OBE, University of Edinburgh professor of infectious disease epidemiology and member of the Scientific Pandemic Influenza Group on Behaviours that advises the British Government. https://www.express.co.uk/life-style/health/1320428/Coronavirus-news-lockdown-mistake-second-wave-Boris-Johnson
[17] https://www.usatoday.com/story/news/health/2020/05/08/coronavirus-pandemic-boosts-suicide-alcohol-drug-death-predictions/3081706001/
[19] Robert Redfield, MD, Director, Centers for Disease Control and Prevention, https://www.buckinstitute.org/covid-webinar-series-transcript-robert-redfield-md/
[22] https://www.researchgate.net/publication/340984562_Estimating_excess_mortality_in_people_with_cancer_and_multimorbidity_in_the_COVID-19_emergency/link/5ea8b957a6fdcc7050976a3e/download
[23]
All of this data was taken from: https://www.usnews.com/news/health-news/articles/2020-07-01/numbers-of-non-covid-19-deaths-up-during-pandemic
[24] https://www.usnews.com/news/health-news/articles/2020-07-01/numbers-of-non-covid-19-deaths-up-during-pandemic
[25] All of the above death total data was taken from: https://www.cdc.gov/nchs/data/databriefs/db355_tables-508.pdf
[26] See, e.g., https://www.lifesitenews.com/news/13-australian-doctors-tell-govt-to-end-lockdowns-theyre-causing-unprecedented-negative-outcomes-1
[28]
https://www.youtube.com/watch?v=blZpgra3XbU
(emphasis added).
[29] https://www.fox35orlando.com/news/fox-35-investigates-questions-raised-after-fatal-motorcycle-crash-listed-as-covid-19-death
[30]
https://www.mlive.com/public-interest/2020/04/medical-experts-say-michigans-coronavirus-death-count-isnt-accurate-but-is-it-too-high-or-too-low.html
[31] https://www.cdc.gov/nchs/data/nvss/coronavirus/Alert-1-Guidance-for-Certifying-COVID-19-Deaths.pdf
[32] https://www.npr.org/sections/coronavirus-live-updates/2020/08/31/907847934/6-million-coronavirus-infections-now-confirmed-in-u-s-a-country-in-limbo (emphasis added).
[33] Washington Post Evening Edition, September 15, 2020, article entitled: Trump health appointee apologizes to HHS staff after accusing scientists of ‘sedition’ (emphasis added).
[35] https://www.aha.org/advisory/2020-04-16-coronavirus-update-cms-releases-guidance-implementing-cares-act-provisions
[36]
See, e.g., one doctor telling a major new outlet this: https://www.youtube.com/watch?v=jB0OYp0S0yo&feature=emb_logo
[39] https://www.uptodate.com/contents/coronavirus-disease-2019-covid-19-critical-care-and-airway-management-issues
[40] Covid-19 — Navigating the Uncharted, by Anthony S. Fauci, M.D., H. Clifford Lane, M.D., and Robert R. Redfield, M.D., New England Journal of Medicine, https://www.nejm.org/doi/full/10.1056/NEJMe2002387 (emphasis added).
[41] The chart is found here: https://data.cdc.gov/NCHS/Conditions-contributing-to-deaths-involving-corona/hk9y-quqm